Family Planning in India: Challenges and Insights from NFHS-4 and NFHS-5
Introduction
Family planning in India has been a cornerstone of the nation’s health and population management policies. While significant progress has been made, the landscape is characterized by regional disparities, socioeconomic inequalities, and cultural nuances. This essay delves into the complexities of family planning practices in India, particularly focusing on urban and rural differences, the role of education and socioeconomic status, cultural influences, and the effectiveness of government interventions. Uttar Pradesh (UP), as a case study, exemplifies the challenges and opportunities inherent in family planning initiatives. Awareness of family planning methods in India is nearly universal, particularly regarding modern methods such as female sterilization and condoms. Studies indicate that women in urban areas and larger cities possess high levels of knowledge about these methods. However, awareness about emergency contraception and female condoms is significantly lower. For instance, only a small proportion of women in Aligarh and Varanasi are familiar with female condoms (Ansary & Anisujjaman, 2012). Despite this widespread awareness, the actual usage of contraceptives remains inconsistent, with a substantial Knowledge, Attitude, and Practice (KAP) gap. This gap is influenced by health concerns, cultural barriers, and limited accessibility to contraceptives in many regions (Singh et al., 2016). Bridging this gap requires a multifaceted approach. Health education campaigns that provide accurate information about contraceptive methods, their usage, and potential side effects are essential. Programs tailored to the unique needs of specific communities can improve adoption rates. These efforts should be accompanied by improving access to contraceptives, particularly for marginalized groups.
The divide between urban and rural areas in family planning practices is stark. While urban populations generally have better access to family planning services, urban slum dwellers face challenges similar to those in rural areas. A study in six cities of UP revealed that slum residents often rely on sterilization or forego contraception altogether, reflecting a lack of access to temporary methods (Speizer et al., 2012). Conversely, rural areas face additional hurdles due to inadequate health infrastructure and cultural conservatism. To address these disparities, investments in health infrastructure are imperative. Rural areas require more community health centers, staffed by trained workers who can offer a variety of contraceptive options. In urban slums, mobile clinics and outreach programs can deliver family planning services directly to those in need. These measures would ensure equitable access to family planning services across geographic and socioeconomic divides.
Socioeconomic factors significantly influence family planning practices. Wealthier and more educated women are more likely to use modern contraceptive methods, while poorer women and those with less education face higher unmet needs for family planning. Education, in particular, plays a transformative role, equipping women with the knowledge to make informed decisions about their reproductive health (Halli et al., 2024). Targeting socioeconomic inequalities requires a multi-pronged strategy. Providing subsidies for contraceptives, expanding public healthcare, and enhancing educational opportunities for women are crucial steps. Empowering women economically and socially can also mitigate the systemic barriers they face. For instance, vocational training programs that improve women’s financial independence can positively influence their family planning choices.
Cultural attitudes and gender norms profoundly impact family planning practices in India. In many northern states, a strong preference for male children continues to shape reproductive behaviors. This cultural norm often results in unintended pregnancies and inhibits the adoption of contraceptive methods. Furthermore, women in patriarchal societies, particularly those with low autonomy, face significant barriers in negotiating family planning decisions (Dyson & Moore, 1983). Challenging these norms requires community-level interventions that engage both men and women. Programs like the “Saas-Bahu Sammelans” (Mother-in-law and Daughter-in-law meetings) have proven effective in fostering discussions around family planning within a culturally sensitive framework (Speizer et al., 2012). Additionally, increasing female autonomy through education and policy interventions can empower women to make decisions about their reproductive health.
The Indian government has undertaken numerous initiatives to enhance family planning services. Programs such as Mission Parivar Vikas aim to increase contraceptive use by focusing on high-fertility states like UP and Bihar. These initiatives emphasize education, availability of diverse contraceptive methods, and community engagement through innovative tools like digital platforms and outreach programs (Sharma et al., 2021). However, the persistence of regional disparities and socioeconomic barriers highlights the need for more nuanced, localized strategies. For greater effectiveness, government policies must be tailored to address the unique needs of various communities. Expanding health infrastructure, particularly in underserved rural and urban slum areas, is critical. Furthermore, male involvement in family planning discussions and decision-making processes can reduce biases and promote shared responsibility in reproductive health. The unmet need for family planning is particularly pronounced among young women aged 15-24, with significant regional disparities across India. Northern states like UP, Bihar, and parts of the northeast exhibit higher unmet needs due to factors such as poverty, low media exposure, and illiteracy. Spatial analyses reveal clusters of unmet needs, emphasizing the importance of targeted resource allocation (Sharma et al., 2021). Addressing these unmet needs requires a focus on education and awareness campaigns that prioritize adolescents and young couples. Geographic targeting, informed by spatial data, can ensure that resources are directed to districts with the highest unmet needs. Offering a variety of contraceptive options and ensuring their availability in these regions are essential steps. Southern states like Kerala and Tamil Nadu exemplify the potential of well-implemented family planning programs. These regions have achieved higher rates of contraceptive use and lower fertility rates due to better education, robust healthcare infrastructure, and greater female autonomy (Joshi et al., 2021). These success stories underscore the importance of investing in women’s education and healthcare as foundational elements of effective family planning. Replicating these successful strategies in states like UP can yield significant benefits. Policies that prioritize women’s empowerment and healthcare investments can bridge the gaps in family planning outcomes across regions.
India’s family planning efforts have achieved progress but continue to grapple with challenges of regional, socioeconomic, and cultural diversity. Bridging the KAP gap, addressing unmet needs, and dismantling cultural barriers are critical to realizing the full potential of these programs. By prioritizing localized interventions, improving infrastructure, and fostering female empowerment, India can achieve equitable and sustainable family planning outcomes. The experiences of successful regions offer a roadmap for scaling best practices, ensuring that no one is left behind in the journey toward better reproductive health and family well-being.
Analysis
Birth spacing, defined as the temporal interval between successive births, plays a crucial role in maternal and child health outcomes. The World Health Organization recommends an optimal birth-to-pregnancy interval of at least 24 months, which translates to a minimum birth-to-birth interval of 33 months when accounting for gestational period (WHO, 2005). This recommendation is supported by substantial empirical evidence demonstrating the positive correlation between adequate birth spacing and improved health outcomes for both mothers and children. Maternal health is significantly impacted by birth spacing intervals. The maternal depletion hypothesis suggests that insufficient intervals between pregnancies prevent women from adequately replenishing their nutritional reserves, which are depleted during pregnancy and lactation. This depletion can lead to maternal undernutrition, compromised body mass index, and increased risk of nutritional deficiencies, particularly anemia (van Eijsden, 2008; Conde Agudelo, 200). Multiple comprehensive studies, including Rutstein’s (2008) analysis of 52 Demographic and Health Surveys and Conde-Agudelo’s (2006) meta-analysis of 67 global studies, have established strong correlations between suboptimal birth spacing and adverse perinatal outcomes. Notably, pregnancies conceived within six months of a previous birth demonstrate a 42-61% higher probability of resulting in low birth weight compared to optimally spaced pregnancies (Wendt, 2012). Furthermore, inter-pregnancy intervals shorter than 18 months significantly increase the risks of preterm birth and small-for-gestational-age (SGA) outcomes. The implications of inadequate birth spacing extend well into childhood development. Research indicates that children born after short birth intervals face substantially higher risks of stunting, wasting, and being underweight. A study in El Salvador demonstrated that children born within 24 months of their siblings had 52% higher odds of stunting compared to those born after longer intervals(Gribble, 2009). These nutritional deficits have long-term consequences. Stunted children frequently experience cognitive delays, reduced educational achievement, and diminished economic productivity in adulthood. Moreover, women who were stunted as children face increased risks during their own pregnancies, perpetuating an intergenerational cycle of undernutrition. The significance of these outcomes is underscored by estimates suggesting that stunting and underweight status each account for approximately 17% of child mortality, while wasting contributes to 11.5% of child deaths (Bhutta, 2013).
| Method | NFHS-4 (%) | NFHS-5 (%) | ||
|---|---|---|---|---|
| Current Use of Family Planning Methods (currently married women age 15–49 years) | Urban | Rural | Urban | Rural |
| Any method | 67.6 | 60.8 | 62.4 | 45.5 |
| Any modern method | 48.6 | 43.2 | 44.5 | 31.7 |
| Female sterilization | 13.5 | 18.0 | 16.9 | 17.3 |
| Male sterilization | 0.1 | 0.1 | 0.1 | 0.1 |
| IUD/PPIUD | 2.1 | 1.3 | 1.5 | 1.2 |
| Pill | 4.4 | 5.4 | 4.4 | 1.9 |
| Condom | 27.1 | 16.6 | 19.1 | 10.8 |
| Injectables | 0.9 | 1.2 | 1.2 | 0.4 |
In NFHS data set the indicator “Current Use of Family Planning Methods (currently married women age 15–49 years)” has the following sub-indicators: Any method, Any modern method, Female sterilization, Male sterilization, IUD?PPIUD, Pill, Condom and Injectables
Where ‘Any method’ includes other methods that are not shown separately; ‘Any modern method’ includes other modern methods that are not shown separately. The evolution of India’s family planning strategy has undergone significant transformations since its inception. While initial contraceptive initiatives encompassed various modern methods, including male sterilization, the program’s focus shifted predominantly toward female sterilization by the late 1970s (de Oliveira IT e al, 2014). The program’s exclusive focus on women persisted through the mid-1990s, reflecting a gender-biased approach to reproductive health services (Singh, 2009).
A paradigm shift occurred in 1998 with the introduction of an informed choice model, eliminating targets and incentives from the family planning framework (de Oliveira IT, 2014). Despite this progressive policy change, contraceptive utilization in India remains influenced by a complex interplay of factors spanning personal, interpersonal, partner-related, service-related, and method-specific dimensions. The challenges in accessing family planning services are particularly pronounced in resource-constrained settings like India, where multiple barriers persist. These include restricted contraceptive options, inadequate service accessibility and quality, cultural and religious opposition, concerns about adverse effects, and deeply embedded gender-based constraints.
| Indicator | NFHS-4 (%) | NFHS-5 (%) | Change |
|---|---|---|---|
| Demand for Family Planning | 66% | 76% | +10% |
| Unmet Need for Family Planning | 13% | 9% | -4% |
| Contraceptive Discontinuation | 33% | 50% | +17% |
The demand for family planning among married women aged 15–49 years has increased significantly, rising from 66% in NFHS-4 to 76% in NFHS-5, reflecting a 10% improvement. This progress has contributed to a reduction in the unmet need for family planning, which has decreased from 13% in NFHS-4 to 9% in NFHS-5. However, a concerning trend has emerged in contraceptive discontinuation rates, which have surged from 33% in NFHS-4 to 50% in NFHS-5, indicating a negative shift (Tripathi, 2023).
Female sterilization remains the predominant contraceptive method in contemporary India, with its adoption significantly influenced by women’s religious background, educational attainment, and occupational status(Jain, 2011; de Oliveira IT et al, 2014). The prevalence of this permanent contraceptive method is further perpetuated by informational deficits and misconceptions regarding temporary contraceptive alternatives.
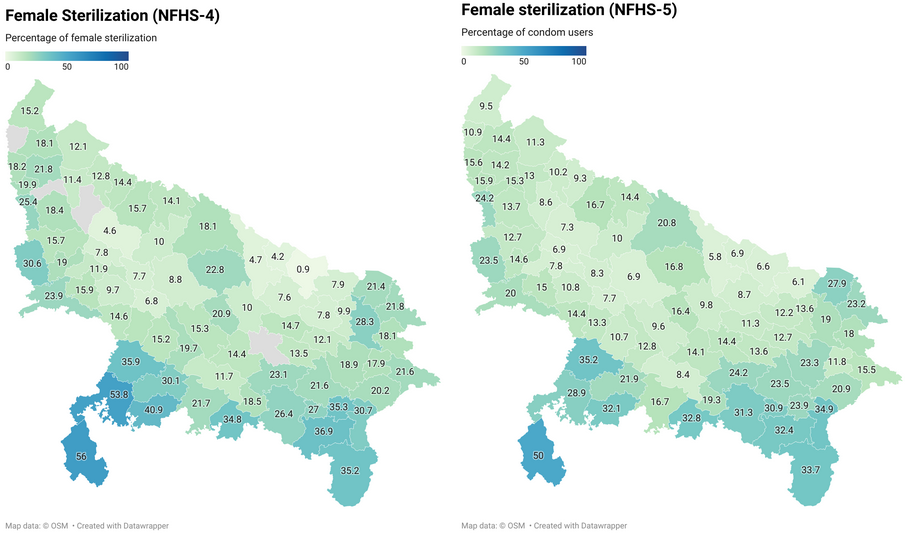
Additionally, the limited accessibility and affordability of modern temporary contraceptive methods often constrain women’s contraceptive choices, inadvertently promoting sterilization as the default option. The situation is further complicated by deeply entrenched socio cultural misconceptions surrounding male sterilization, particularly the erroneous beliefs that vasectomy diminishes sexual desire and compromises physical strength. As can be seen in table 1, where the female sterilization percentage for both rural 18% and urban areas 13% is drastically more than the percentage of male sterilization (Rural and Urban= 0.1%). This hasn’t changed over the years when the NFHS-5 survey is compared to NFHS-4 survey. For both NFHS-4 and NFHS-5 total male sterilizations amounts to 0.1%. Misconceptions contribute significantly to the public’s resistance toward male sterilization as a viable contraceptive alternative, thereby reinforcing the disproportionate burden of contraceptive responsibility on women (Perry, 2016). According to a qualitative study conducted among women in Mumbai’s low-income neighborhoods, poor women believe that choosing to get sterilized helps them effectively manage their fertility, which improves their emotional and sexual well-being after the procedure. Most of them have no regret after sterilization because of all these circumstances (Brault, 2016). In Uttar pradesh majority of the states show a drop in female sterilization percentage indicating a rise in usage of other modern methods including IUD, pills, contraceptive and injectables.
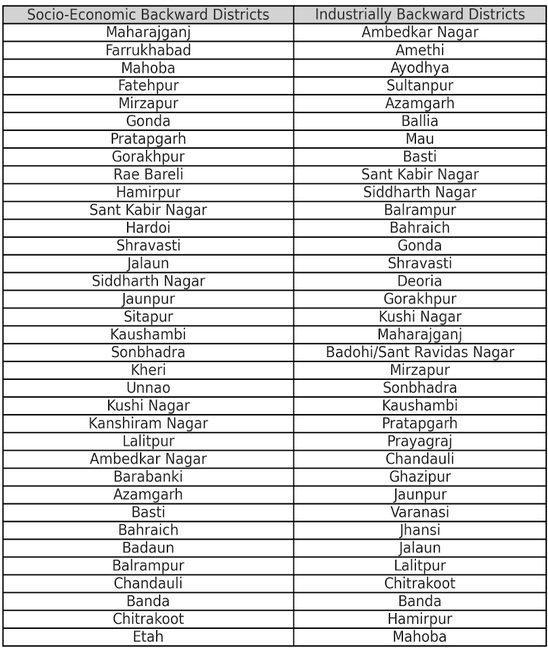
Socioeconomic Backwardness and Family Planning
Uttar Pradesh has 35 districts notified as industrially and socio-economically backward. The University Grants Commission has identified 55 out of the existing 70 districts of Uttar Pradesh as backward which are below the national average in total literacy based on the 2001 census.
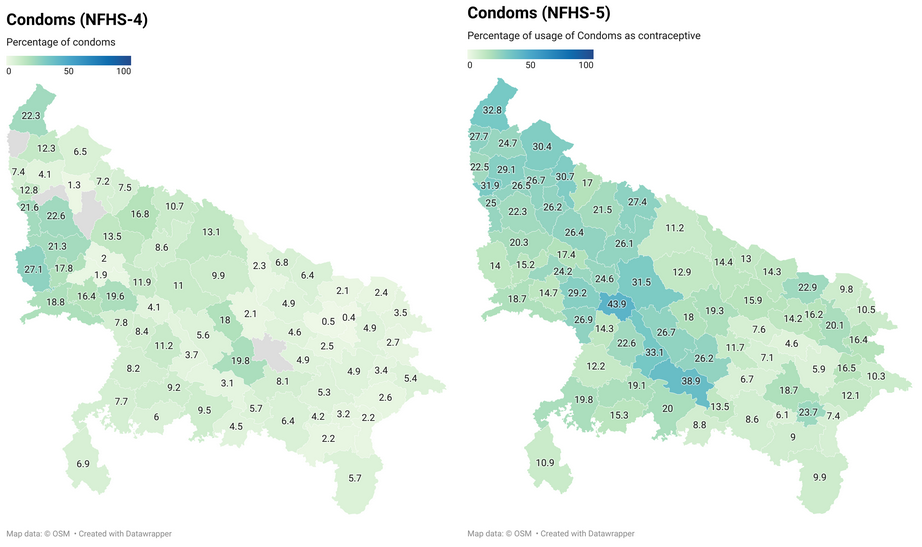
Even with huge rural backwardness NFHS-5 data doesn’t show much rural-urban divide between the usage of condoms, pills, IUD/PPIUD (%) and injectables or any other modern methods as can be seen in Figure 1.
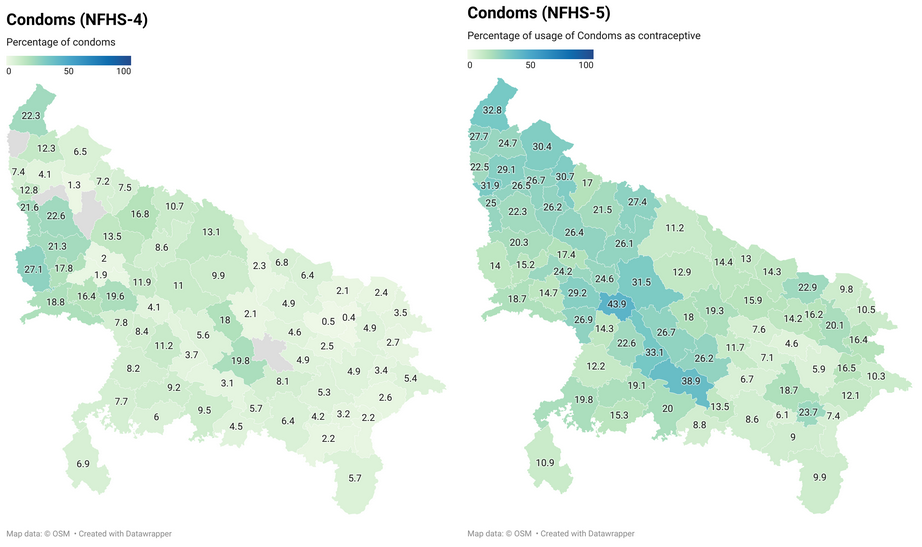
Modern methods used other than the ones mentioned have increased all over in multiple districts as you can see in Figure 3. According to HMIS reports available with the Ministry of Health and Family Welfare, the National Family Welfare Program has been implemented satisfactorily, with IUCD insertions rising from 52,75,440 to 55,40,743 and sterilisations rising from 40,30,409 to 40,70,597 between 2014–15 and 2015–16. In accordance with the National Population Policy, 2000’s policy framework for population stabilization, family planning has been a top priority for the government and has been actively promoted through the National Rural Health Mission, which was established in 2005. Addressing the unmet need for contraception and reaching a stable population by 2045—at a level compatible with the demands of social development, sustainable economic growth, and environmental protection—were the primary goals of the National Population Policy of 2000. The nation’s Total Fertility Rate (TFR) decreased from 2.7 in 2006 to 2.2 in 2016 as a result of government programs (NFHS-IV). Between 1990 and 2000, the decadal growth rate was 21.54 percent; between 2001 and 2011, it was 17.64 percent. Out of 36 states and territories, 24 have already attained the replacement level TFR of 2.1 or below, and the crude birth rate has decreased from 23.8 in 2005 to 20.8 (SRS 2015). Such government interventions have played a key role in usage of modern methods and techniques for family planning.
Conclusion
The landscape of family planning in India is shaped by a complex interplay of regional, socioeconomic, and cultural factors. While significant strides have been made, challenges persist, particularly in bridging the gaps in awareness, accessibility, and adoption of contraceptive methods. Rural-urban disparities highlight the necessity of targeted interventions tailored to the needs of diverse populations. Investments in healthcare infrastructure, particularly in underserved areas, are essential for equitable access to family planning resources. Education and socioeconomic empowerment emerge as transformative forces in improving family planning outcomes. Educated and economically independent women are better equipped to make informed decisions about their reproductive health. Consequently, policies that prioritize women’s education and provide financial support for contraceptive use are critical. Addressing entrenched cultural norms and gender biases, particularly in patriarchal regions, requires community engagement initiatives that foster dialogue and shared decision-making between men and women. Government initiatives like Mission Parivar Vikas underscore the importance of localized, data-driven strategies in addressing unmet family planning needs. By focusing on high-fertility regions and employing innovative outreach tools, such programs have laid the groundwork for progress. However, the persistence of issues like low male participation and high contraceptive discontinuation rates necessitates a more inclusive approach that balances the responsibility of family planning between genders.
–
References
Ansary, R., & Anisujjaman, M. (2012). Factors determining pattern of unmet need for family planning in Uttar Pradesh, India.
Bhutta, Z. A., Das, J. K., Rizvi, A., Gaffey, M. F., Walker, N., Horton, S., Webb, P., Lartey, A., & Black, R. E. (2013). Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? The Lancet, 382(9890), 452–477. https://doi.org/10.1016/S0140-6736(13)60996-4
Brault, M. A., Schensul, S. L., Singh, R., Verma, R. K., & Jadhav, K. (2016). Multilevel perspectives on female sterilization in low-income communities in Mumbai, India. Qualitative Health Research, 26(11), 1550–1560. https://doi.org/10.1177/1049732315580556
Conde-Agudelo, A., & Belizan, J. M. (2000). Maternal morbidity and mortality associated with interpregnancy interval: Cross sectional study. British Medical Journal, 321(7271), 1255–1259. https://doi.org/10.1136/bmj.321.7271.1255
Conde-Agudelo, A., Rosas-Bermúdez, A., & Kafury-Goeta, A. C. (2006). Birth spacing and risk of adverse perinatal outcomes: A meta-analysis. JAMA, 295(15), 1809–1823. https://doi.org/10.1001/jama.295.15.1809
de Oliveira, I. T., Dias, J. G., & Padmadas, S. S. (2014). Dominance of sterilization and alternative choices of contraception in India: An appraisal of the socioeconomic impact. PLOS ONE, 9(1), e86654. https://doi.org/10.1371/journal.pone.0086654
Dyson, T., & Moore, M. (1983). On kinship structure, female autonomy, and demographic behavior in India. Population and Development Review, 9(1), 35–60. https://doi.org/10.2307/1972894
Gribble, J. N., Murray, N. J., & Menotti, E. P. (2009). Reconsidering childhood undernutrition: Can birth spacing make a difference? An analysis of the 2002–2003 El Salvador National Family Health Survey. Maternal & Child Nutrition, 5(1), 49–63. https://doi.org/10.1111/j.1740-8709.2008.00161.x
Halli, S. S., Alam, M. T., Namasivayam, V., Prakash, R., Anand, P., Blanchard, J., & Wehrmeister, F. (2024). Geographic and socioeconomic inequalities in the coverage of contraception in Uttar Pradesh, India.
Jain, R., & Muralidhar, S. (2011). Contraceptive methods: Needs, options and utilization. The Journal of Obstetrics and Gynecology of India, 61, 626–634. https://doi.org/10.1007/s13224-011-0107-7
Joshi, S., Uttamacharya, Borkotoky, K., Gautam, A., Datta, N., Achyut, P., & Nanda, P. (2021). Spatial variation in contraceptive practice across the districts of India, 1998–2016.
Perry, B., Packer, C., Chin-Quee, D. S., Zan, T., Dulli, L., & Shattuck, D. (2016). Recent experiences and lessons learned in vasectomy programming in low-resource settings: A document review.
Rutstein, S. O. (2008). Further evidence of the effects of preceding birth intervals on neonatal, infant, and under-five-years mortality and nutritional status in developing countries: Evidence from the Demographic and Health Surveys. Macro International Inc.
Sharma, H., Singh, S. K., & Srivastava, S. (2021). Spatial heterogeneity and major correlates of unmet need of family planning among young married women aged 15–24 in India: An exploratory study.
Singh, A., & Ram, F. (2009). Men’s involvement during pregnancy and childbirth: Evidence from rural Ahmadnagar, India. Population Review, 48(1), 83–102.
Singh, A., Singh, K. K., & Verma, P. (2016). Knowledge, attitude and practice gap in family planning usage: An analysis of selected cities of Uttar Pradesh.
Speizer, I. S., Nanda, P., Achyut, P., Pillai, G., & Guilkey, D. K. (2012). Family planning use among urban poor women from six cities of Uttar Pradesh, India.
Tripathi, S., Pathak, V. K., & Lahariya, C. (2023). Key findings from NFHS-5 India report: Observing trends of health indicators between NFHS-4 and NFHS-5. Journal of Family Medicine and Primary Care, 12(9), 1759–1763. https://doi.org/10.4103/jfmpc.jfmpc_246_23
van Eijsden, M., Smits, L. J., van der Wal, M. F., & Bonsel, G. J. (2008). Association between short interpregnancy intervals and term birth weight: The role of folate depletion. The American Journal of Clinical Nutrition, 88(1), 147–153. https://doi.org/10.1093/ajcn/88.1.147
Wendt, A., Gibbs, C. M., Peters, S., & Hogue, C. J. (2012). Impact of increasing inter-pregnancy interval on maternal and infant health. Paediatric and Perinatal Epidemiology, 26(Suppl 1), 239–258. https://doi.org/10.1111/j.1365-3016.2012.01285.x
World Health Organization. (2005). Report of a WHO consultation on birth spacing. WHO.
Data Sources:
- National Family Health Survey (NFHS-4 and NFHS-5)
- Health Management Information System (HMIS)
- Ministry of Health and Family Welfare, Government of India
- World Health Organization Guidelines
This analysis was conducted as part of the MPP232: Rural Development Policy course at Christ (Deemed to be University).